
Diagnosis and Test Sleep Apnea
How Is Sleep Apnea Diagnosed?
A diagnosis of sleep apnea can only be made after a sleep study confirms you are experiencing breathing problems in your sleep. In order to determine whether you should be referred for a sleep study, a doctor will first perform a physical exam, ask about symptoms, and collect your personal and family history.
During an evaluation for sleep apnea, a doctor may ask one or more of the following questions:
Do you feel tired or sleepy during the day?
Has anyone told you that you snore or have pauses in breathing during your sleep?
Is it difficult to stay awake performing tasks like driving, reading, or watching TV?
Do you currently smoke, or have you smoked in the past?
Has anyone in your family been diagnosed with sleep apnea?
During the exam, the doctor may also take into consideration whether your weight, neck circumference, or blood pressure, or other medical conditions put you at higher risk of sleep apnea. Some doctors may request that you fill out a questionnaire about your sleep habits.
If the doctor suspects sleep apnea based on your exam and symptoms, they will likely recommend that you have a sleep study.
Polysomnogram
A polysomnogram is a sleep study in which medical sensors are used to monitor a person’s breathing, heart rate, and the electrical activity of their brain waves while they sleep. A person must have a polysomnogram, either in a sleep lab or at home, in order to be diagnosed with sleep apnea.
If you have a polysomnogram at a sleep lab, your health care provider will give you instructions on when to arrive, what to bring with you, and whether you should make any changes to your diet or medications that day.
After acclimating to your room at a sleep lab, a technician attaches monitoring sensors to your legs, fingers, chest, and head. The sensors measure body processes while you sleep. The data are then translated into stages of sleep, wakefulness, and events where breathing is interrupted.
If the doctor thinks it’s very likely that you have sleep apnea, they may order a sleep study with the potential to trial a positive air pressure (PAP) device. This is called a split-night sleep study. If the polysomnogram results from the first half of the night confirm that you have significant sleep apnea, a PAP device will be applied and customized in the second half of the night to help prepare you for ongoing treatment.
A PAP device helps keep the soft tissues of the airway open by routing pressurized and humidified air through a tube and mask fitted to your face while you sleep. Your physiological activity is monitored at different air pressures provided by the PAP device to see which is the best pressure for you.
A polysomnogram at a sleep center may be preferred over a home sleep apnea test if you have heart or lung disease, risk factors for central sleep apnea or potential to be diagnosed with other sleep disorders.
Home Sleep Apnea Tests
A home sleep apnea test (HSAT) may be an option for people who are suspected of having moderate to severe obstructive sleep apnea based on their symptoms, medical history, and physical exam. An HSAT takes fewer measurements than an in-lab sleep study, and does not have brain sensors (EEG) and muscle sensors (EMG) that measure sleep or sleep stages.
That said, home sleep apnea tests do provide some benefits. For example, when a person sleeps in the comfort of their own home, they are more likely to have longer periods of sleep. An HSAT can also be used to help determine whether a PAP device is working well or to reevaluate a person if they are still experiencing symptoms after starting treatment.
Different home sleep apnea test kits are available and your sleep doctor will instruct you on the proper application of the sensors.
After you take a test, your doctor reviews the data and works with you to provide the best course of treatment.
Diagnostic Criteria
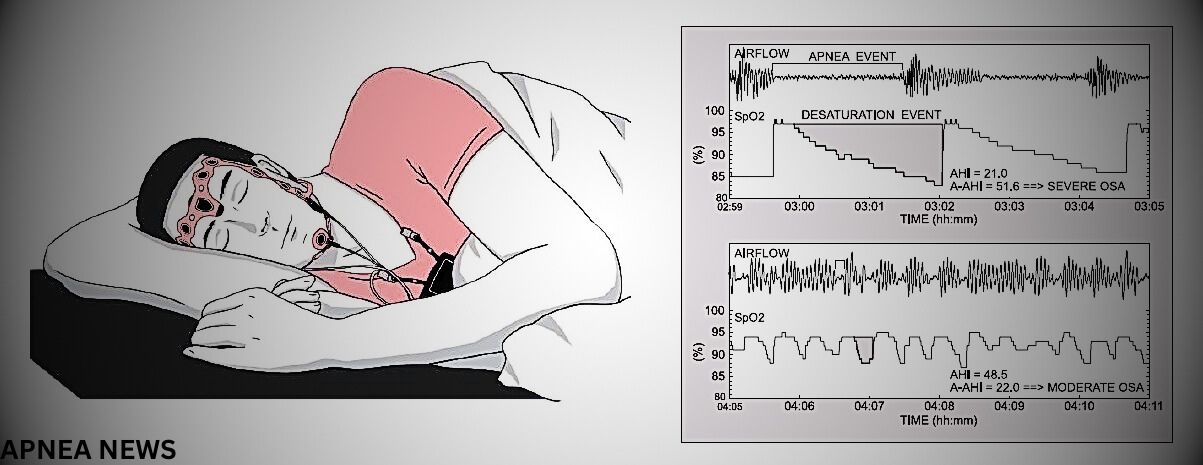
A diagnosis of obstructive sleep apnea is based on the results of the polysomnogram and the presence or absence of certain symptoms. A polysomnogram records how many apneas, hypopneas, or respiratory effort-related arousals (RERA) occur per hour while a person is asleep.
Apnea: Apnea is when airflow stops for a period of 10 seconds or longer.
Hypopnea: Hypopnea is a period of shallow breathing that lasts for at least 10 seconds and causes a drop in the oxygen level in your blood or a brief arousal from sleep.
Respiratory effort-related arousal (RERA): RERAs occur when breathing is restricted more subtly than a hypopnea but is still associated with a brief arousal from sleep.
Common symptoms of sleep apnea include daytime sleepiness, snoring, and morning headaches. Less commonly, people may experience insomnia or nighttime awakenings with an urge to use the bathroom.
Sleep apnea is diagnosed if at least 5 breathing events per hour of sleep are recorded during the sleep study. The severity of sleep apnea is primarily determined by the average number of breathing events per hour and, combined with symptoms and medical history, is used to inform treatment options.
A diagnosis of central sleep apnea also requires careful consideration of a person’s symptoms and polysomnography results. However, there are several subtypes of central sleep apnea, and each has specific diagnostic criteria.
Next Steps After Getting a Diagnosis
If you are diagnosed with sleep apnea, a member of your health care team will explain what type of sleep apnea you have and whether the condition is mild, moderate, or severe. They may also talk about some of the potential health risks associated with sleep apnea and offer precautions against driving if you are frequently sleepy during the day.
Next, a doctor will discuss what kind of treatment is appropriate for your situation. The treatment plan will depend upon what type of sleep apnea you have and the severity of the disorder, as well as your personal preferences.
For most people, sleep apnea is a chronic condition. This means that ongoing treatment usually alleviates symptoms, but stopping treatment will cause the condition to come back. Over time, it is common for sleep apnea to slowly get worse.
For most people, sleep apnea can be managed effectively with a combination of medical treatment and healthy sleep habits.
Positive airway pressure therapy: PAP therapy is a primary treatment option for OSA and certain types of CSA. A PAP device has a maskthat is worn over your nose and mouth during sleep. The mask is connected by a hose to a small machine beside your bed, and the machine pumps air through the hose and mask to open your airway.
Other breathing devices: Apart from PAP, there are also oral appliances that position your tongue or jaw in a way that doesn’t block airflow. These oral appliances may be considered for some people as an alternative treatment to PAP therapy.
Healthy sleep habits: Regular physical activity, losing weight, and maintaining healthy sleep habits may relieve symptoms of sleep apnea. Changing sleep position from lying on your side to lying on your back may also help.
Surgery: Surgical treatment may be an option for some people. The goal of surgery is to stabilize or enlarge the upper airway in order to improve airflow. It is hard to predict who will respond well to a surgical procedure, and it is common for residual OSA to persist. In this case, the surgery may make PAP therapy more tolerable and effective.
Nerve stimulation: Another option for people who are not able to tolerate PAP therapy is a surgically implanted devicein the upper chest. This device connects to a nerve that pushes the tongue forward with breathing in order to help clear the airway. Multiple criteria must be satisfied to pursue this type of treatment for obstructive sleep apnea.
Possible Signs of Sleep Apnea
Sleep apnea may present itself in a number of ways. Consider talking with your doctor if you have one or more symptoms of the condition.
Daytime sleepiness:Daytime sleepiness includes feelings of low energy or poor focus. People with sleep apnea may also unintentionally fall asleep during daytime activities.
Loud snoring or gasping for air during sleep: A partner or a family member may notice that you are snoring or experiencing shallow or irregular breathing.
Morning headaches: Morning headaches that occur daily or multiple times a week are reported by some people with obstructive sleep apnea.
Sleep-maintenance insomnia: Waking up multiple times in the night can be a symptom of sleep apnea. Repeated awakenings may lead to more urges to urinate in the night.
Risk Factors for Sleep Apnea
A risk factor is anything that increases the likelihood a person will develop a health problem. Risk factors for sleep apnea include personal characteristics and family history.
Large neck circumference: A neck with a circumference greater than 17 inches for men and 15.5 inches for women may indicate excess fat, including tongue fat, that could narrow or block the airway.
Age: Individuals older than 65 are at higher risk for central sleep apnea.
Misaligned jaw:A small lower jaw or an abnormally shaped upper jaw may impact positioning of the tongue, which in turn can block the airway during sleep.
Family history of snoring and apnea: The risk of developing obstructive sleep apnea is approximately 50% greater if a first-degree relative such as a sibling or parent has the condition.
Sleep apnea is also more likely to occur in people that have certain health conditions. People with cardiac conditions, including high blood pressure and heart failure, commonly have sleep apnea.
Untreated sleep apnea can affect a person’s quality of sleep and daily life. However, timely diagnosis and treatment for sleep apnea can prevent complications and relieve symptoms in most cases.